
Caldwell-Luc Surgery
- Dr. Zibran Khan

- Jul 16, 2019
- 2 min read
Updated: Jan 22, 2022
I was called in to consult for a case where the distobuccal root of the Maxillary left Third molar was pushed accidentally into the maxillary sinus.
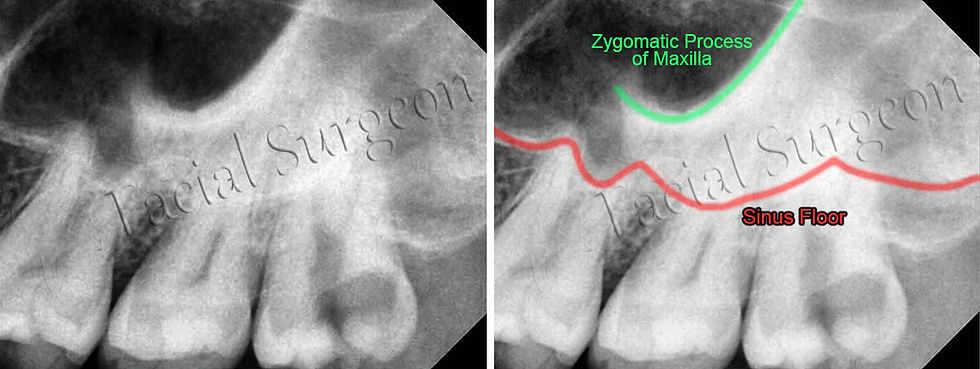
Below is the preop IOPA of the Maxillary left Third molar. Zygomatic process of Maxilla was mistaken as Maxillary sinus floor by the general dentist.
Displacement of tooth root into the maxillary sinus leads to two problems.
1. Oro-Antral Communication (OAC) was created in Maxillary left Third molar region. If left untreated then it may lead to Oro-Antral Fistula which would further lead to Maxillary sinusitis.
2. The root of a carious tooth was pushed into the maxillary sinus which would lead to sinusitis if not managed immediately.

The patient was informed of the root in the sinus and OAC. The patient wanted to get the root removed as soon as possible.
Caldwell-Luc Surgery was planned followed by OAC closure in Maxillary left Third molar region.

The nerve blocks administered were Infraorbital Nerve Block, Posterior Superior Nerve Block and Greater palatine Nerve Block. An additional Local infiltration at the site of incision was done to reduce intra-op bleeding.

The flap raised was a Trapezoidal Flap with mesial releasing incision given mesial to the canine and distal releasing incision given distal to the second premolar.
A semilunar incision is preferable in this case. As I was performing a Caldwell-Luc surgery after a long time, I completely forgot about this incision.

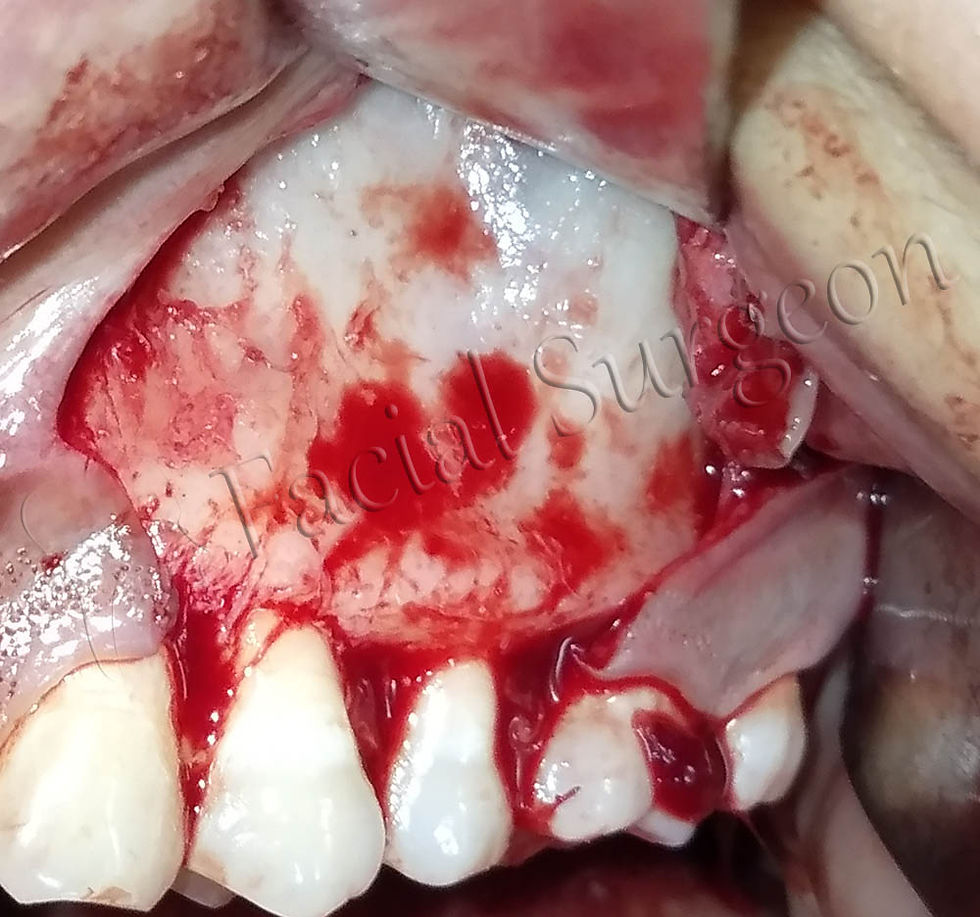
After the flap was raised, a window was created in the region approximately 5 mm apical to the roots of canine and first premolar. The created window was of the width of roughly the diameter of an index finger.


After exploring the sinus for some time, the root piece was visible from the window.
An artery forcep was used to remove the root piece from the Maxillary sinus.

Once the root was removed the sinus was irrigated with betadine.
Initially, I planned to close the Schneiderian membrane using 5-0 Vicryl Rapide suture. But it was not available at the clinic so I left the membrane as it is and proceeded to close the oral mucosa.
Watertight Mucosal Flap closure was done using 3-0 Silk suture with simple interrupted sutures.

Then I proceeded to close the OAC using the Buccal Advancement flap (Rehrmann Flap).
An anterior releasing incision was given mesial to Maxillary left Third molar and flap reflected properly to view the periosteum.

Then a horizontal incision was given in the periosteum to free the mucosa to be extended over the extraction socket.
Watertight closure of the flap was done using 3-0 Silk suture with simple interrupted sutures.
Water Holding test was performed to check the efficacy of the closure. As expected, there was no nasal regurgitation of water.
So, the patient was discharged from the clinic.
I tried taking pictures of the OAC closure but the pictures didn't turn up to be article worthy. Accessibility and visibility in the region is limited and that lead to bad pictures.
The patient was prescribed Antibiotic, Analgesic, Antihistaminic and steam inhalation to prevent sinusitis.
The patient is recalled after 3 days for follow-up and after two weeks for suture removal.


Click here provide members with discounts on over-the-counter medications, vitamins, and health essentials, promoting better health management and cost-effective wellness solutions. kaiserotcbenefits.com - more details here
Click here help you find recent death notices, providing information about funeral services, memorials, and tributes for loved ones in your area. obituariesnearme.com - more details here
Click here? Many users have had mixed experiences with the platform, so it's important to read reviews and verify deals before booking. istravelurolegit.com - more details here